Stem Cells in Myeloid Neoplasms and Bone Marrow Failure
Cammenga Group
Our Research
Our lab has a long-standing interest in the molecular pathogenesis of myeloid neoplasms (acute myeloid leukemia and myelodysplastic syndrome).
We have performed studies to investigate the role of hypoxia and the transcription factor hypoxia inducible factor 1 alpha (HIF-1alpha) in AML and myeloproliferative neoplasms as well as in the response to chemotherapy of AML.
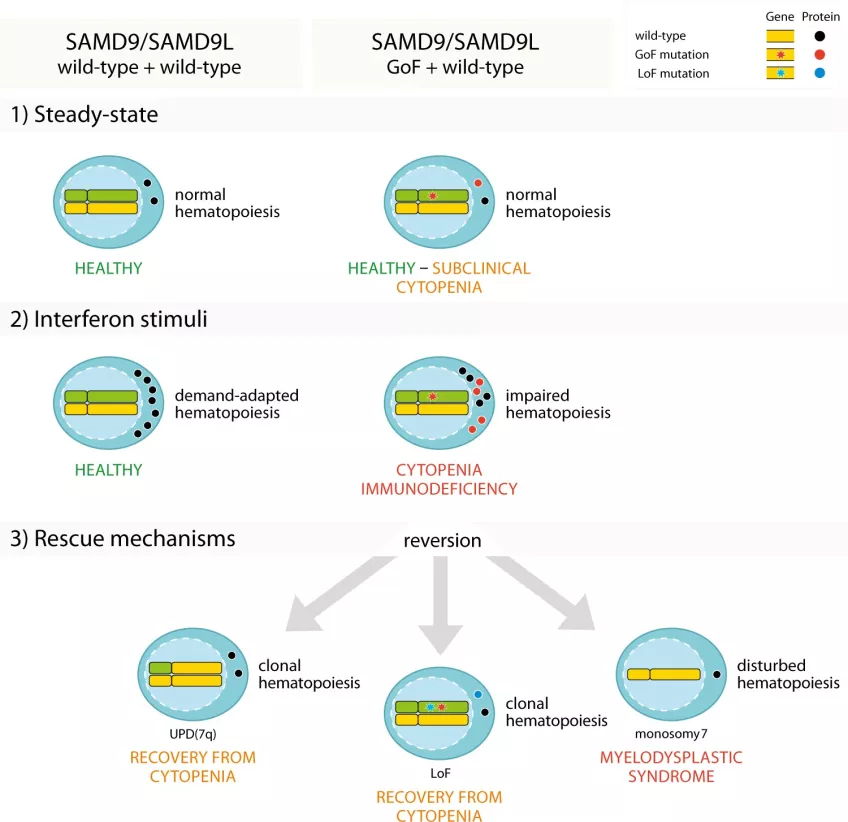
In a collaboration with Dr. Y. Bryceson we identified germline gain of function mutations in SAMD9L as a cause of bone marrow failure and myeloid neoplasms with monosomy 7 and we were the first to show the different mechanisms of primary somatic genetic reversion (SGR) in individuals with germ-line gain of function (GOF) SAMD9L mutations. The three different mechanisms of primary somatic genetic reversion are uniparental disomy (UPD) of chromosome 7q, loss of function mutations in cis or “adaption by aneuploidy” by monosomy 7 or der(1;7) resulting in myeloid neoplasms (Figure 1).
In collaboration with Dr. J. Maciejewski’s group at the Cleveland Clinic we have also identified germline loss-of function SAMD9/SAMD9L mutations in adult patients with myeloid neoplasms.
Because myeloid neoplasms are the major indication for allogeneic hematopoietic stem cell transplantation, we also try to understand the molecular mechanisms of relapse after transplantation.
Aims
- To identify and understand the basis of genetic predisposition to myeloid neoplasms
- To identify therapeutic targets in myeloid neoplasms
- To improve outcome of allogeneic hematopoietic stem cell transplantation
Impact
Genetic predisposition to myeloid neoplasms has recently been included in the latest WHO classification of myeloid neoplasms. It is currently assumed that 5-10% of all myeloid malignancies are caused by a genetic predisposition and that probably half of the mutations causing a predisposition to myeloid neoplasms have been identified. Individuals with a genetic predisposition to myeloid neoplasms normally develop leukemia earlier in life than patients without a predisposition.
Our work has contributed to the understanding of the ataxia pancytopenia syndrome (ATXPC, OMIM159550), the myelodysplasia and leukemia syndrome with monosomy 7 (MLSM7, OMIM 252270), refractory cytopenia of childhood (RCC), transient monosomy 7 and a subgroup of inherited bone marrow failures.
Team
Jörg Cammenga
Principal Investigator, Jorg [dot] Cammenga [at] med [dot] lu [dot] se (Jorg[dot]Cammenga[at]med[dot]lu[dot]se)
Alexandra Rundberg-Nilsson
Postdoc, Alexandra [dot] Rundberg_Nilsson [at] med [dot] lu [dot] se (Alexandra[dot]Rundberg_Nilsson[at]med[dot]lu[dot]se)
Gustav Rydstrom
Guest Researcher, gustav [dot] rydstrom [at] med [dot] lu [dot] se (gustav[dot]rydstrom[at]med[dot]lu[dot]se)
Jörg Cammenga

Principal Investigator
PhD, Professor
Division of Molecular Medicine & Gene Therapy
Department of Laboratory Medicine
Lund Stem Cell Center
BMC B14, Lund University
221 84 Lund, Sweden
Phone: + 46 46 222 85 79
Mail:Jorg [dot] Cammenga [at] med [dot] lu [dot] se (Jorg[dot]Cammenga[at]med[dot]lu[dot]se)
Current Major Grants
- Cancerfonden
- Barncancerfonden